
{kind=link}

WHO Recommends Near-Point-of-Care Tests, Tongue Swabs, and Sputum Pooling to Revolutionize Tuberculosis Diagnosis
The World Health Organization (WHO) has issued groundbreaking new guidance that expands the global toolkit for diagnosing tuberculosis (TB) introducing near-point-of-care molecular tests, the use of tongue-swab samples, and sputum-pooling strategies to make testing faster, simpler, and more cost-efficient. Released on 9 March 2026, these recommendations mark the most significant update to TB diagnostics in nearly a decade and are expected to transform early detection efforts, especially in resource-limited settings.
Closing the Persistent Diagnostic Gap
TB remains one of the world’s top infectious killers. Despite decades of progress, millions of people still go undiagnosed or receive a diagnosis only after long delays. WHO’s End TB Strategy and the UN High-Level Meeting on TB committed countries to ensure universal access to rapid diagnostics yet only a fraction of those infected currently benefit from modern testing.
The new recommendations aim to change that. They address specific bottlenecks that keep testing out of reach for too many people:
- Dependence on laboratory instruments located far from communities
- Exclusive reliance on sputum samples, which some patients cannot produce
- High costs of equipment and supplies that limit expansion beyond urban centers
Dr Tereza Kasaeva, Director of WHO’s Department for HIV, TB, Hepatitis & STIs, stated: “These new recommendations mark a major step forward in making TB testing faster and more accessible. WHO urges countries and partners to roll out these guidelines to close persistent diagnostic gaps and ensure that everyone with TB can be diagnosed early and start life-saving treatment without delay.”
The Three Major Innovations
Near-Point-of-Care (NPOC) Molecular Tests
For the first time, WHO is recommending a class of near-point-of-care nucleic acid amplification tests (NPOC-NAATs) that can detect TB at the periphery of the health system including small laboratories, primary health-care centers, and mobile clinics.
Unlike conventional molecular instruments previously limited to central labs, NPOC devices are portable, battery-operated, and lower in cost. They provide results within hours, bridging the gap between mass screening and rapid diagnosis in remote or humanitarian settings. Initial evaluation showed comparable accuracy to existing low-complexity automated assays for detecting TB in adults and adolescents.
This expansion supports countries where rural patients often travel days to reach diagnosis. Early confirmation at community level prevents transmission and improves treatment outcomes. The approach echoes principles seen in preventive checkups bringing essential screening closer to where people live.
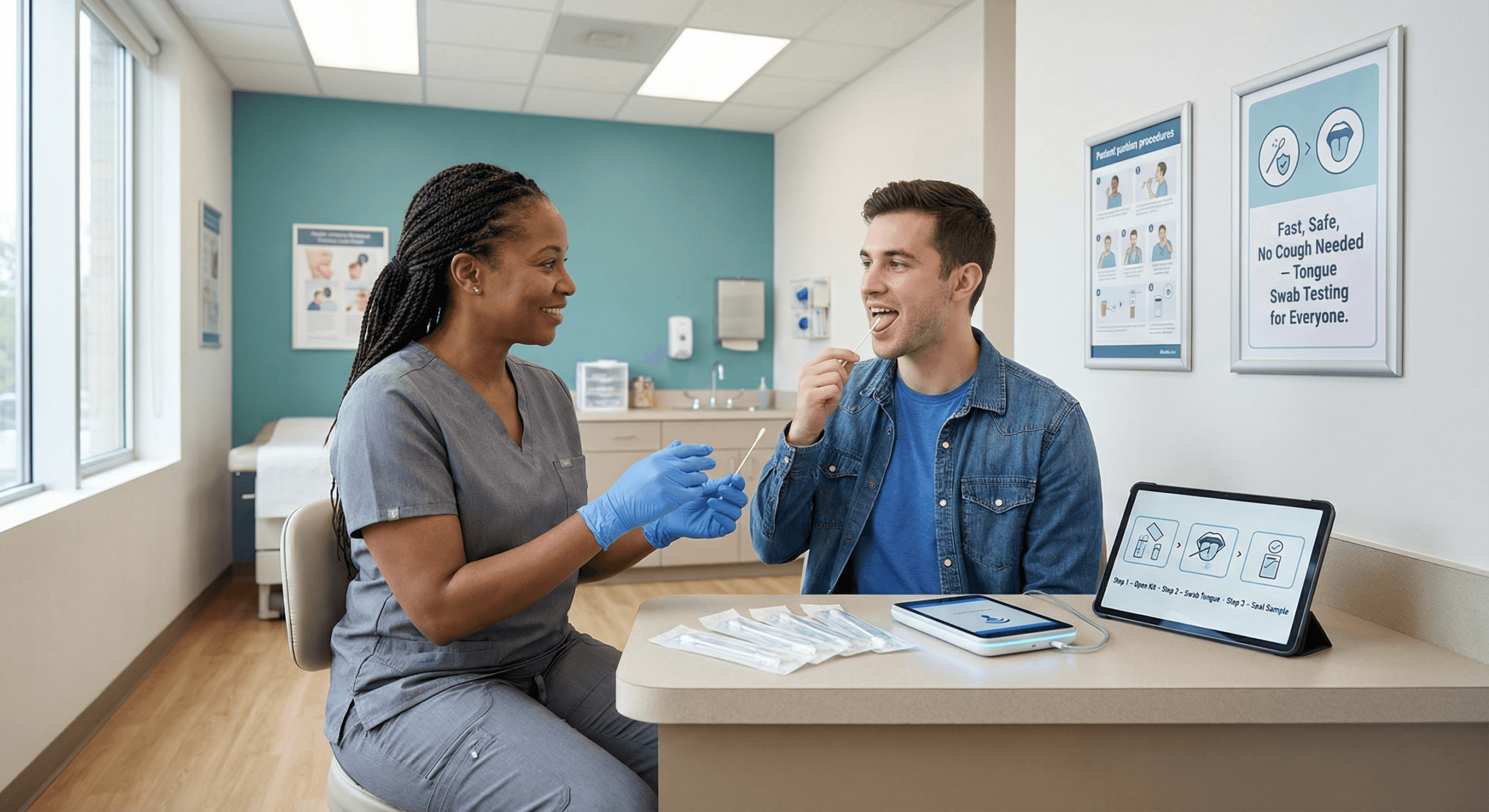
Tongue-Swab Samples
Traditional TB diagnosis relies on expectoration of sputum a barrier for children, aged people, and many HIV-positive patients. WHO now endorses tongue swabs as a new, non-invasive specimen type for use with both NPOC-NAATs and LC-aNAATs.
The simple method uses a sterile swab rubbed along the dorsal surface of the tongue to collect saliva and mucosal cells where Mycobacterium tuberculosis DNA can be detected. This innovation is expected to:
- Enable testing of populations unable to produce sputum
- Simplify collection in outpatient or home settings
- Allow rapid screening in schools, prisons, and refugee camps without aerosol exposure risks
By reducing discomfort and stigma, tongue swabs may encourage earlier presentation for testing a critical factor in high-burden countries where diagnostic delays fuel ongoing transmission.
Pooling of Sputum Samples
To stretch resources further, WHO is introducing sputum pooling as a cost-saving strategy for detecting TB and rifampicin resistance. Multiple samples from different individuals are combined and tested as one batch using validated LC-aNAAT systems. If a pooled sample tests positive, each individual sample is then retested separately.
When infection rates are low, this approach can cut testing costs by 30–50 percent while maintaining sensitivity. It also increases throughput in situations where reagents or technicians are limited, such as during disease surges or outbreaks.
Evidence, Guidelines, and Next Steps
The updates are based on a systematic review and meta-analysis conducted between 2024 and 2025 under the GRADE framework (Grading of Recommendations, Assessment, Development and Evaluation). They will appear in the new edition of WHO’s Consolidated Guidelines on Tuberculosis: Module 3 (Diagnosis), 2nd Edition, to be published later this year along with an updated Operational Handbook.
These documents provide step-by-step implementation guidance on technologies, specimen types, and testing algorithms. An accompanying Toolkit for Near-Point-of-Care and Swab-Based Testing will offer customizable planning tools, training materials, and monitoring frameworks. To aid roll-out, WHO and partner organizations plan regional webinars and interactive resources through the WHO TB Knowledge-Sharing Platform.
National TB programmes are encouraged to seek WHO technical assistance before purchasing devices or adapting protocols, ensuring alignment with quality standards and biosafety requirements.
Implications at Different Levels
Local and Community Impact
At the frontline of care, these recommendations can dramatically expand access. A health worker in a rural clinic will soon be able to perform molecular testing onsite, delivering results within the same visit. Patients who previously traveled long distances or awaited lab referrals will start treatment immediately limiting transmission to family members and co-workers.
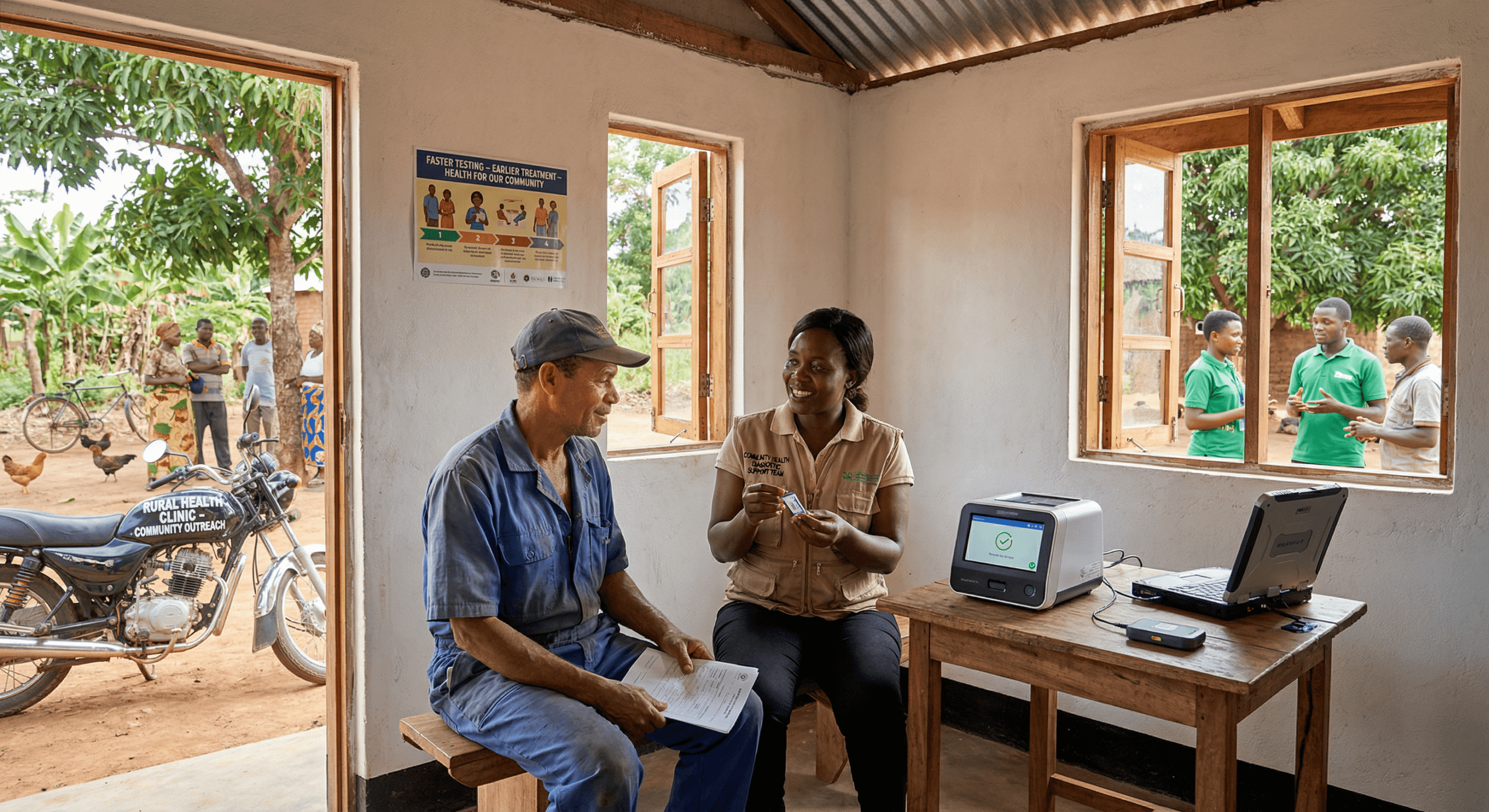
Tongue swabs require no electricity, refrigeration, or special training beyond basic infection-control measures, making them ideal for community-screening campaigns. Pooling techniques can stretch budget allocations in small district hospitals where every cartridge counts.
For patients, these advances translate directly into equity: those in remote areas, children, older adults, people with HIV, and health-care workers in fragile settings will all gain access to timely, accurate diagnosis.
National Health System Implications
Nationally, the new technologies can transform how TB programmes are organized. Countries that integrate NPOC testing into primary care networks will see faster case detection rates and reduced burden on central laboratories. Lower-cost devices will fit within Universal Health Coverage budgets and reduce financial dependency on external donors.
Ministries of Health will need to revise national testing algorithms, train front-line staff, and ensure supply chains for swabs and cartridges. Linking diagnostic data to digital systems will allow real-time surveillance and rapid mapping of drug-resistance patterns a major advantage for planning drug procurement and preventing outbreaks of rifampicin-resistant TB.
Economic models suggest that wider testing using pooling methods could yield long-term savings for national health budgets, reducing hospitalization costs through earlier diagnosis and shorter infectious periods.
Regional and Continental Effects
Across regions, adoption of near-point-of-care testing could narrow the gap between high-burden and low-burden countries. Regional reference laboratories may shift from routine screening to complex drug-resistance testing and quality assurance. This redistribution of tasks will strengthen capacity throughout the network and improve precision in cross-border surveillance.
Continental health bodies such as the Africa CDC and the Pan American Health Organization can use the new tools to harmonize standard operating procedures and training across member states. Joint procurement and shared maintenance agreements may further reduce costs and ensure supply security, especially during global shortages of diagnostic reagents.
Global Public-Health Significance
At the global level, these recommendations are seen as essential to achieving the End TB Strategy goal of reducing TB deaths by 90 percent by 2035. Diagnostic innovation is arguably the weakest link in current control efforts; these updates directly address it.
Simpler and faster diagnosis also has security implications. Every undiagnosed case serves as a potential source of infection, fueling transmission within crowded urban slums or displacement camps. By bringing testing closer to communities, countries can curtail chains of infection before they cross borders.
The shift to swab-based collection reduces reliance on cough-inducing procedures that generate infectious aerosols, increasing safety for health-care workers. Pooling methods reflect an emerging ethos in global health optimizing efficiency without sacrificing accuracy.
Global partners such as the Stop TB Partnership and the Global Fund are expected to incorporate these recommendations into grant support criteria, accelerating market availability. Public-private collaboration may also expand production capacity so that smaller-scale manufacturers across continents can meet demand.
Scientific and Operational Perspectives
For researchers, these recommendations open fresh avenues of study. Tongue-swab sampling may lead to new understanding of mycobacterial biology in the oral microbiome, while data from pooling strategies can improve epidemiological modeling and resource allocation.
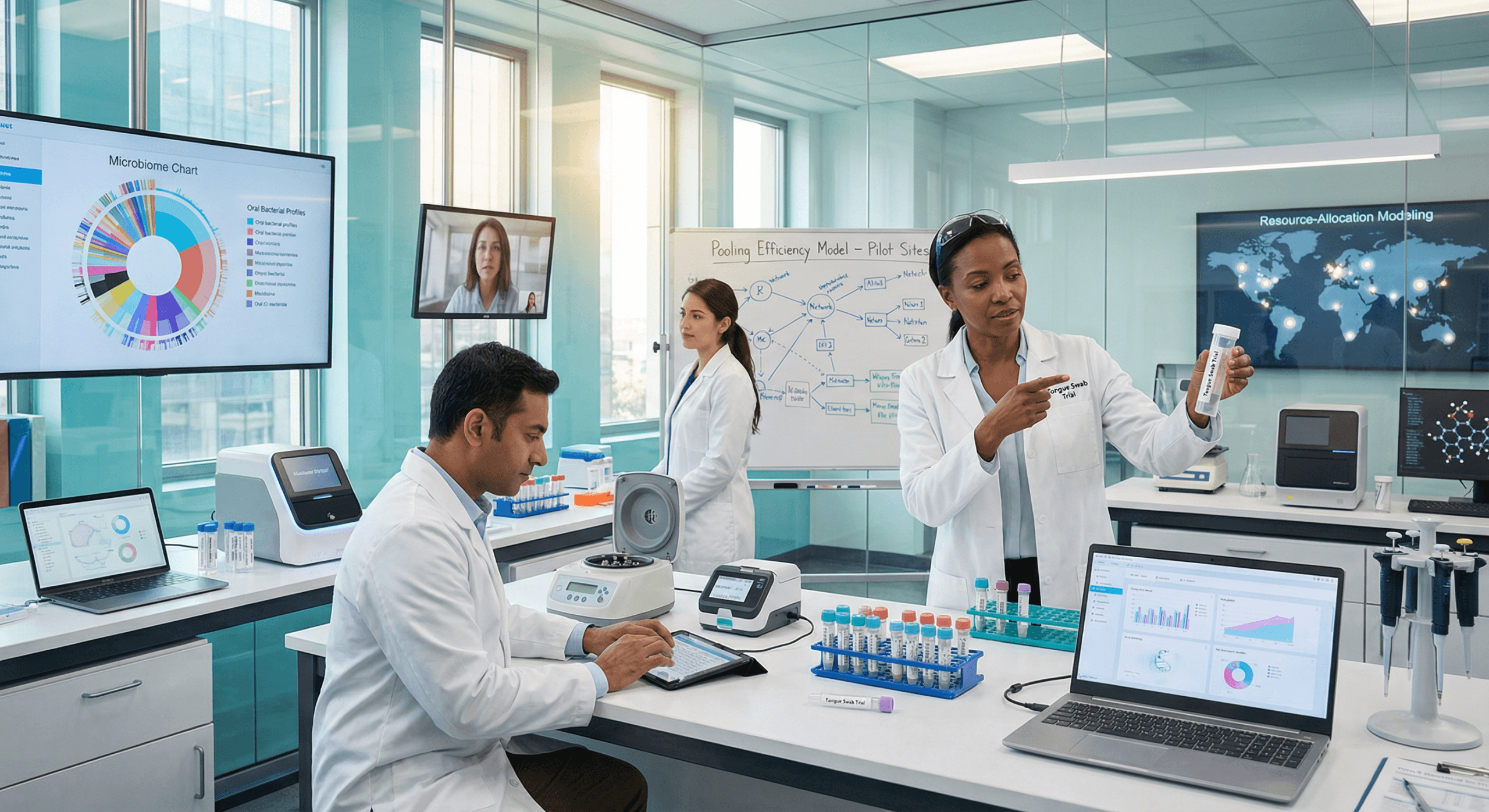
Operational research will be critical in validating cost-effectiveness across different epidemic intensities. WHO encourages Member States to contribute findings to a global repository to inform future updates of its TB Diagnostic Modules.
Looking Ahead: Implementation and Support
The release of these recommendations marks only the first step in a broader implementation effort. WHO’s upcoming Operational Handbook will guide countries in planning budgets, evaluating readiness, and training laboratory personnel. It will also include model algorithms connecting diagnostic pathways to clinical management for both drug-sensitive and drug-resistant TB.
Furthermore, the new Toolkit will provide templates for logistics tracking, quality-control audits, and supervision checklists to help programmes monitor performance. When combined with real-time data from digital platforms, these resources will form a comprehensive ecosystem for continuous improvement in TB diagnosis.
Implementation will be phased by country capacity, but WHO expects early adopters in Asia and Africa to begin piloting NPOC and swab-based testing within months. Demonstration projects coordinated with national reference laboratories will generate operational lessons for scale-up.
The Bigger Picture: Equity Through Innovation
TB disproportionately affects low- and middle-income countries, where diagnostic infrastructure is scarce. The WHO guidance represents not just a technical update but a commitment to health equity. By simplifying testing and reducing cost per result, these technologies can help close one of the most persistent inequities in infectious-disease care.
If implemented broadly, analysts predict millions of additional people could receive accurate diagnoses each year a development that would significantly reduce TB transmission, accelerate progress toward eradication goals, and save countless lives worldwide.
Summary
WHO released new recommendations (9 March 2026) introducing near-point-of-care molecular tests, tongue-swab sampling, and sputum-pooling strategies for TB and drug-resistant TB diagnosis. These methods aim to close diagnostic gaps, lower costs, and extend testing to peripheral and community levels. NPOC tests enable on-site molecular diagnosis within hours; tongue swabs simplify collection for those unable to provide sputum; pooling maximizes efficiency and reduces reagent use. A new Operational Handbook and Toolkit will guide countries in deployment, training, and quality assurance. The recommendations carry implications at local, national, regional, and global levels advancing equity and supporting the End TB Strategy goals for 2035.
This content is for educational purposes and does not substitute for professional psychological or therapeutic help.