When Healers Need Healing: What Two Nurses Learned on the Other Side of Care
A particular kind of disorientation comes from finding yourself in an unexpected role. This feels especially true when you know that role intimately from the outside. For those who spend their professional lives caring for others, becoming the one who needs care can feel like stepping through a mirror into a world that’s familiar yet fundamentally altered.
Jenny and Shar understood patient care deeply. Both experienced cardiac nurses, they had spent years supporting people through frightening diagnoses. They explained treatment options and offered calm presence during medical crises. They knew the clinical language, the protocols, and the emotional landscape of illness. Neither anticipated how profoundly different that landscape would feel when they became the travelers rather than the guides.
Their story isn’t about heroism or silver linings. It’s about the uncomfortable education that comes from vulnerability. It explores what shifts inside us when we must receive the kind of care we’ve always given.
The Conversation That Changed Everything
The day Shar asked to speak privately, Jenny expected a work issue. Perhaps a scheduling conflict or a clinical question would come up. Instead, Shar shared news that felt surreal. A routine mammogram had led to additional imaging, then a biopsy, and finally a diagnosis of breast cancer. Healthy, active, with no family history, Shar was still processing the cognitive dissonance of a diagnosis that didn’t match her self-concept.
As Jenny listened, she felt her chest tighten. Her left arm began to ache. Her smartwatch buzzed with an elevated heart rate alert. The discomfort was unfamiliar and unsettling, but her first instinct was dismissal. Probably just anxiety, she told herself. A stress response to difficult news about someone she cared about.
Shar noticed the hesitation and asked gentle questions. She reflected back what Jenny was describing. She stayed present rather than rushing to reassurance. Both women had used this approach countless times with patients who minimized symptoms that deserved attention.
Research on health-seeking behavior consistently demonstrates something important. We are remarkably skilled at explaining away symptoms that don’t fit our narrative about ourselves. Studies in the Journal of the American Heart Association note that women often attribute cardiac symptoms to anxiety or stress. Heart disease doesn’t align with how they see themselves, and the symptoms can be ambiguous.
Jenny eventually agreed to go to the emergency department, but only if Shar came with her. The role reversal had already begun. This resistance to seeking care mirrors patterns discussed in emotional hygiene daily habits. We protect our emotional equilibrium by minimizing signals that something needs attention.
Recognizing Yourself in the Patient Experience
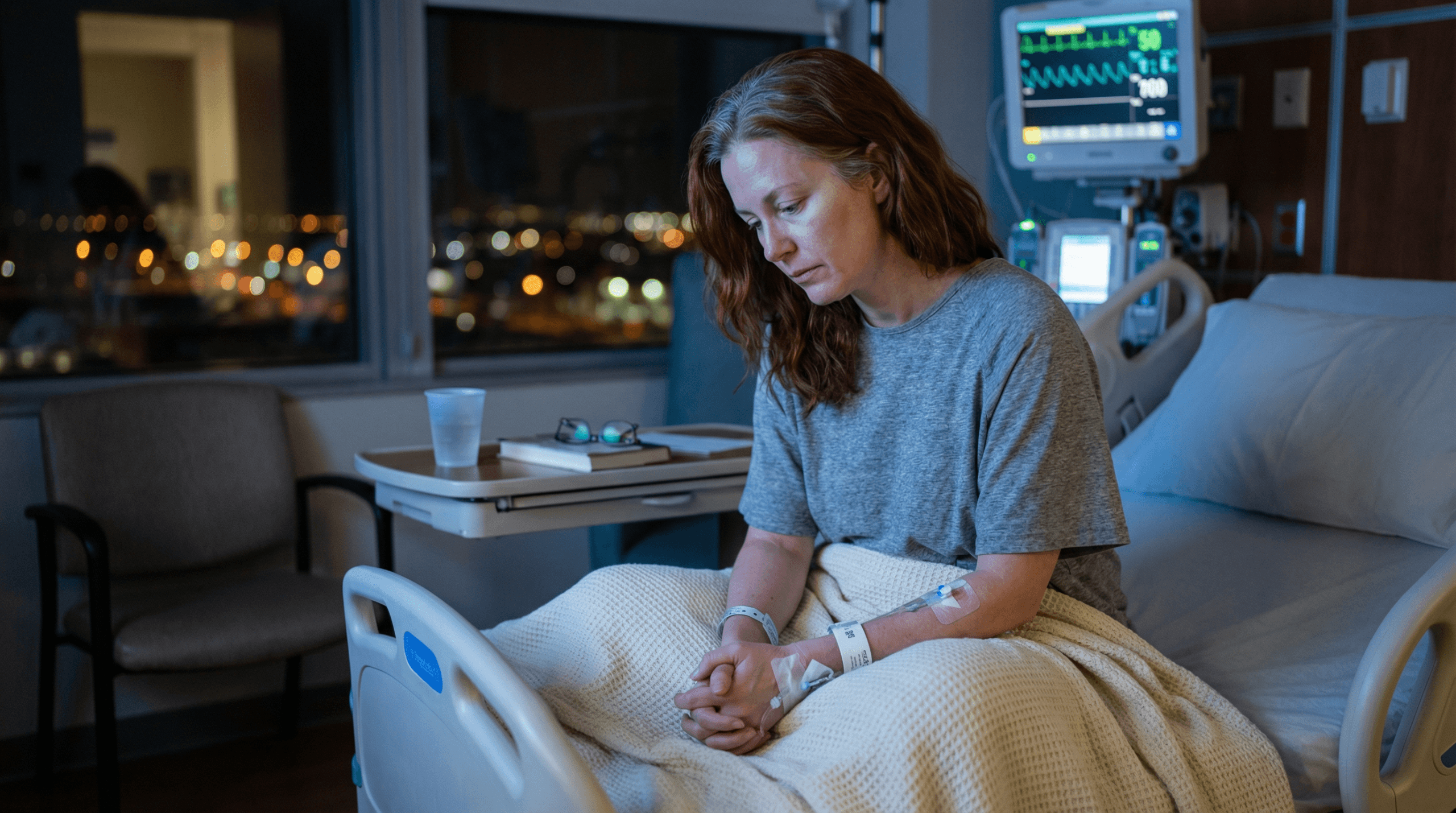
Within hours, Jenny was in the cardiac catheterization lab. She knew this space well but had never experienced it from the procedure table. Doctors diagnosed her with spontaneous coronary artery dissection (SCAD). This rare and often misunderstood condition causes heart attacks and disproportionately affects younger, otherwise healthy women. Jenny required stents, intensive monitoring, and days in the coronary care unit.
The diagnosis didn’t match anything Jenny had imagined for herself. She exercised regularly and understood cardiovascular health. She had cared for heart patients for over a decade. Yet none of that knowledge insulated her from the emotional shock of suddenly becoming a cardiac patient. Understanding the facts about blood pressure and heart health didn’t erase the fear of experiencing cardiac distress firsthand.
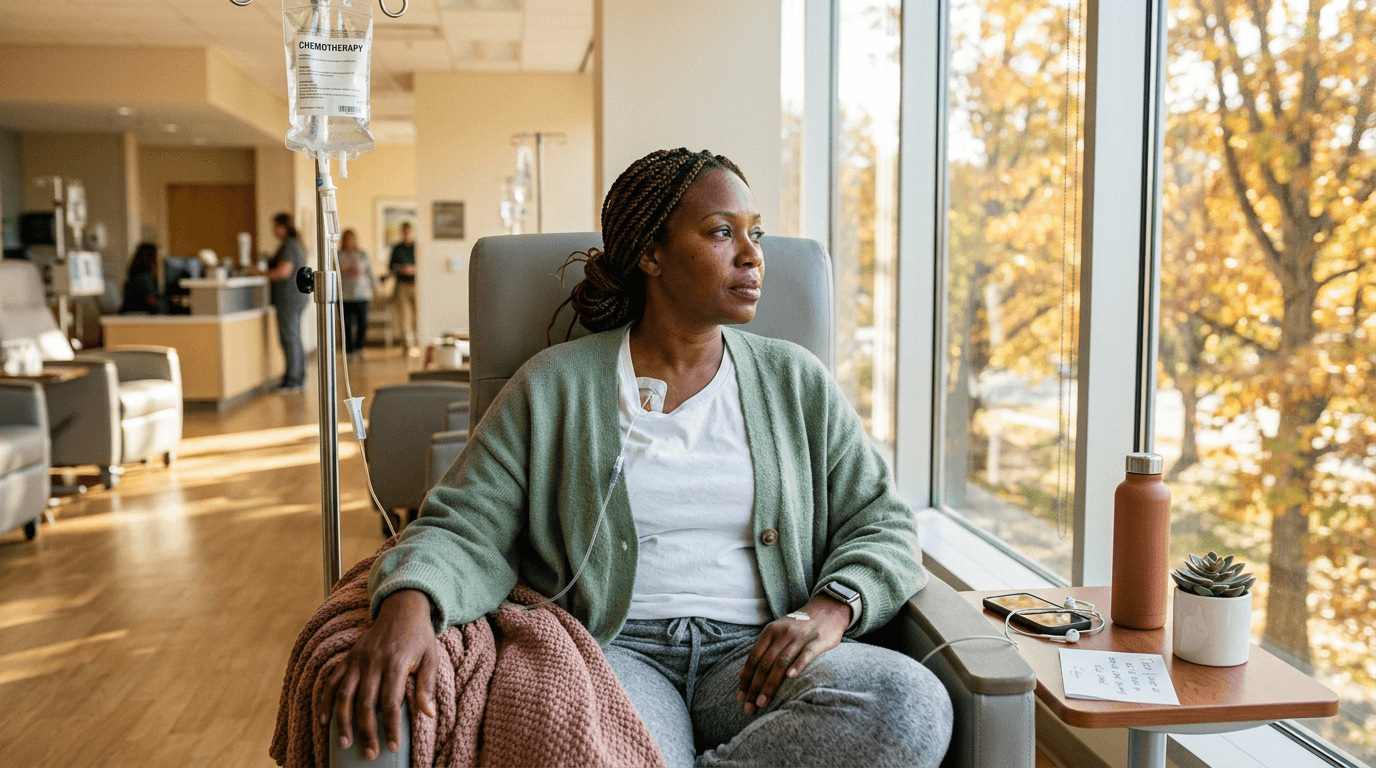
Shar, meanwhile, was beginning her own treatment journey. Chemotherapy, immune therapy, and the physical toll of cancer care awaited her. Both women were learning what it meant to move through the healthcare system not as experts, but as people whose bodies had become unfamiliar.
What struck them both wasn’t the competence of their care. They received excellent treatment. Instead, the internal experience of receiving it surprised them most. The loss of control stood out. So did the waiting and the difficulty of asking for help. A strange guilt emerged from needing support when you’re used to providing it.
What Shifts When You’re the One Being Cared For
For caregivers, the transition to patient can surface uncomfortable truths about identity and worth. When so much of your self-concept is built around being competent and needed, illness can feel like a failure rather than a circumstance.
Research on caregiver identity from the American Journal of Nursing suggests that helping professionals often struggle with role confusion when they become care recipients. The internalized belief that asking for help equals weakness can delay treatment-seeking and complicate recovery.
Both Jenny and Shar noticed this pattern in themselves. They had to consciously practice what they’d always encouraged in patients. Acknowledging limits became essential. Accepting support required daily effort. Allowing others to step into the caretaking role demanded a kind of emotional maturity that felt harder to access when they were the vulnerable ones.
Their professional perspective also began to shift. Jenny found herself reconsidering how she explained procedures to patients. What language actually landed? What created more anxiety? Shar noticed how much energy it took to maintain composure during treatment. She appreciated colleagues who didn’t require her to perform wellness she didn’t feel.
The shift wasn’t dramatic or sudden. It was cumulative. A series of small recalibrations reshaped how they understood care and vulnerability. This ongoing adjustment reflects the same emotional regulation skills needed to navigate any major life transition.
The Lessons That Only Vulnerability Can Teach
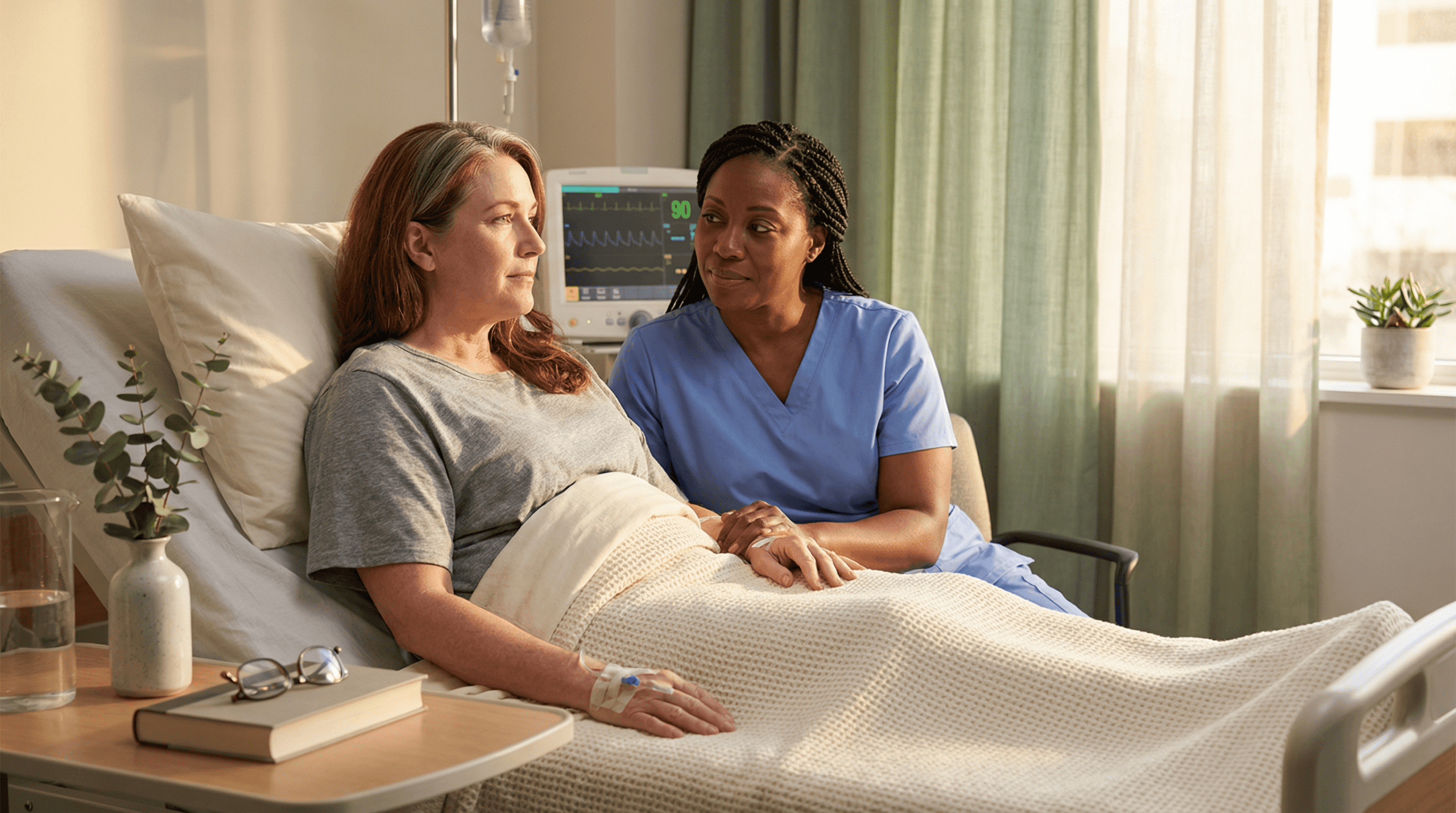
As their treatment paths unfolded, Jenny and Shar supported each other in quiet, practical ways. Shar showed up to Jenny’s cardiac rehabilitation sessions. She didn’t come to coach or advise, but simply to be present. Jenny checked in before and after Shar’s chemotherapy appointments. She understood the particular anxiety of waiting for test results.
What emerged wasn’t a tidy narrative of mutual inspiration. Something more grounded developed instead. They recognized that serious illness humbles everyone, regardless of expertise. Humor and honesty matter more than forced positivity. Being seen in your struggle without having to minimize or explain it is itself a form of care.
Their friendship deepened not because of their diagnoses. It grew because they allowed themselves to be genuinely vulnerable with each other. They didn’t perform resilience or rush toward meaning-making. They made space for difficulty without trying to fix it. This kind of emotional safety became foundational to their recovery process.
According to APA research on social support and health, perceived social support correlates strongly with recovery outcomes. Support that allows authentic emotional expression matters most. Quality of presence outweighs quantity of intervention.

Reflection: When Your Identity and Your Circumstances Collide
Jenny and Shar’s story raises questions worth sitting with. These reflections matter especially for those whose identities are closely tied to competence or self-sufficiency.
What parts of your self-concept depend on always being the capable one? When that capability is compromised through illness or loss, what happens to your sense of self?
How comfortable are you receiving care without performing gratitude? Many of us can accept help only if we immediately reciprocate or downplay its significance. This pattern often reflects deeper beliefs explored in redefining strength beyond the unbreakable myth.
Do you extend to yourself the same compassion you offer others? Holding ourselves to standards of resilience we would never impose on loved ones is common. Developing self-compassion and a balanced self-image can help close this gap.
These aren’t questions with immediate answers. They invite you to notice the gap between how you think you’d respond to vulnerability and how you actually do.
Moving Forward, Changed
Both women continue their treatment and recovery. Jenny monitors her cardiac health with new awareness. She has become more attuned to the difference between normal fatigue and concerning symptoms. Shar is progressing through radiation and immune therapy. She maintains both realism and hope about her prognosis.
They remain nurses still knowledgeable, still skilled, still committed to patient care. But their understanding of what care means has shifted. They’re more attuned to the emotional labor of being a patient. They recognize how much courage it takes to show up for treatment when exhausted or afraid. They notice the quiet dignity in people navigating circumstances they didn’t choose.
The experience didn’t grant them special wisdom or transform their suffering into meaning. It simply gave them a perspective they couldn’t have accessed any other way. From the other side of care, competence and knowledge provide some comfort. But they don’t eliminate fear or uncertainty.
Takeaway
Becoming the person who needs help requires emotional maturity that can only develop through lived experience. This is especially true when you’re accustomed to providing care for others. It asks you to release the identity built around self-sufficiency. It challenges you to practice the vulnerability you’ve encouraged in others. For Jenny and Shar, that transition wasn’t about finding silver linings in illness. It was about allowing themselves to be fully human in their struggle. They found connection in shared honesty rather than performed strength. The lesson isn’t that suffering teaches us. It’s that how we hold ourselves and each other through difficulty shapes what becomes possible on the other side.
This content is for educational purposes and does not substitute for professional psychological or therapeutic help.