Building Healthspan, Not Just Lifespan: What the Next Decade of Your Health Actually Depends On
There is a particular moment that many adults in their mid-40s or early 50s describe in similar terms. It is not a diagnosis, it is not a crisis, it is the quiet recognition, often arriving through watching someone else, that the question was never simply how long. A parent navigating their late 70s with chronic limitation that began accumulating two decades earlier. A colleague whose cardiac event arrived without warning at 54. A decade of professional peak that traded physical capacity for output, with terms nobody read carefully. Understanding what healthspan after 40 actually means, and what drives it, is where the most consequential health decisions of midlife begin.
After that recognition, the conversation most longevity content offers feels inadequate. More years is not the goal. The goal is what those years contain.
Lifespan and Healthspan After 40: The Distinction That Changes Everything
Healthspan is the portion of a life spent in genuine functional health, with the physical capacity, metabolic stability, cognitive clarity, and mobility to do what matters without significant limitation. Lifespan is simply the count of years a life lasts.
| Lifespan | Healthspan | |
|---|---|---|
| What it measures | Total years alive | Years of functional independence and physical capacity |
| Primary driver | Genetics, medical care, circumstance | Behavioral patterns, particularly in midlife |
| Point of leverage | Limited individual influence | High, especially in the decade of 42 to 62 |
| What decline looks like | Death | Progressive loss of capacity, mobility, and independence |
The National Institute on Aging identifies healthspan as the central challenge of aging research, specifically how to compress the period of chronic disease and functional limitation into the shortest possible window at the end of a long life. That compression is not automatic. The research is consistent in identifying it as substantially a behavioral outcome.
What Functional Health Measures vs. What Lifespan Counts
Lifespan research has extended the count considerably. What it has not resolved is what fills those additional years. Healthspan research asks a different question: not how long can we survive, but how long can we sustain the functional capacity to live rather than merely persist.
The distinction between the two is most visible not in clinical data but in the lived experience of people who spend their final decade in meaningful engagement versus those who spend it managing the accumulated consequences of earlier decades. Protecting functional quality of life is a goal that midlife behavioral patterns either serve or erode, often quietly, over years.
Where the Gap Opens After 40 and Why This Decade Is the Inflection Point
After 40, adults who reached midlife with comparable physical baselines begin separating into meaningfully different functional trajectories. Muscle mass declines at roughly one to two percent per year after 50 without countervailing resistance training, according to research synthesized by the American College of Sports Medicine. VO2 max, the measure of aerobic capacity that a landmark study in JAMA Network Open identified as among the strongest predictors of all-cause mortality, declines at approximately ten percent per decade in sedentary adults. Insulin sensitivity begins shifting in ways closely tied to behavioral patterns rather than age alone.
The midlife window matters because these declines compound. Behavioral investment at 48 does not merely help. It operates on a longer timeline, from a higher starting position, with adaptation capacity that diminishes as the decades advance. For anyone thinking seriously about functional aging, the 40s and early 50s represent the highest-leverage window available.
The Physical Domains Healthspan After 40 Actually Protects
Healthspan in your 40s and 50s is not a single metric. It is the sustained function of several interconnected physical systems, each with its own trajectory and its own vulnerability in midlife.
Muscle Mass and Cardiovascular Fitness the Two Domains With the Highest Midlife Leverage
Sarcopenia, the age-related loss of muscle mass and strength, is among the most consequential and most underestimated physical changes of midlife. What begins as modest decline in the 40s accelerates after 50 and carries downstream effects well beyond physical appearance: reduced metabolic rate, significantly higher fall risk, decreased functional independence, and measurably higher all-cause mortality in longitudinal research.

The ACSM’s position on muscle mass in aging adults is direct. Resistance training is the primary intervention, and the evidence behind it is among the most durable in exercise science. This is not new information. It is information that professional demands and the cultural invisibility of sarcopenia have kept from receiving the urgency it warrants.
Cardiovascular fitness carries independent predictive weight that most adults in this demographic underestimate. Adequate VO2 max determines whether a 57-year-old can sustain a weekend of physical activity without spending the following week recovering, manage a flight delay involving three terminal changes, or bring the physical reserves to family life that professional peak years routinely consume. Fitness is not an aesthetic variable at this stage. It is a functional one.
Metabolic Flexibility, Mobility, and Cognitive Function What Determines Independence in Later Decades
Metabolic flexibility, the body’s capacity to shift efficiently between glucose and fat as fuel sources, declines with age and sedentary behavior in ways closely tied to insulin sensitivity. Research in this area consistently associates reduced metabolic flexibility with elevated risk of chronic metabolic disease and cognitive impairment over time.
Adults managing prediabetes or existing metabolic conditions should work with their care team rather than apply general behavioral guidance to clinical situations requiring individualized management.
Mobility, the combination of joint range of motion, balance, and functional movement patterns, determines whether a person at 72 rises from the floor independently or navigates uneven terrain without risk. Among all healthspan domains, mobility responds well to consistent attention in midlife and degrades rapidly during the years when professional demands crowd it out. The cost of neglect here is paid in later decades with compounding interest.
The Behavioral Practices With the Strongest Evidence for Healthy Aging After 40
This is where the healthspan conversation most often either dissolves into vague encouragement or overcorrects into protocols requiring clinical infrastructure, expensive equipment, and time that working adults in their late 40s and 50s do not have. Neither serves the adult who understands the stakes and is looking for what is actually actionable from where they are.
The practices with the strongest evidence are specific. They are not particularly complex. They are available without expensive protocols, supplements, or tracking systems that add overhead without adding outcomes.
Resistance Training and Zone 2 Cardio the Two Practices Most Midlife Adults Underinvest In
Resistance training performed two to three times per week, with sufficient load to stimulate muscle adaptation, is the primary behavioral intervention for preserving muscle mass and functional strength through midlife. The ACSM recommends progressive resistance training for all healthy adults, with particular emphasis after 50 given the accelerating rate of sarcopenia at that threshold.
The entry point for a previously sedentary adult is not a complex program. Two sessions per week covering major muscle groups with progressive challenge over time fits within the genuine constraints of a demanding professional life and produces meaningful protective return.
Zone 2 cardiovascular training, sustained aerobic effort at moderate intensity where conversation is possible but requires some effort, builds mitochondrial density and aerobic base in ways that support both daily functional capacity and the VO2 max trajectory most sedentary midlife adults are losing faster than they recognize. Three sessions of 30 to 45 minutes across most weeks produces meaningful adaptation for adults without existing cardiovascular conditions.
Adults with existing cardiovascular, musculoskeletal, or metabolic conditions should consult their healthcare provider before initiating or significantly modifying exercise or nutrition patterns. For adults who have been sedentary for extended periods, a baseline assessment before beginning resistance training or more intensive cardiovascular work is sound clinical practice.
Protein Intake, Sleep, and Stress Regulation the Supporting Architecture Most Adults Undervalue
Protein intake becomes a more consequential variable after 50, when muscle protein synthesis requires both higher total intake and better distribution across meals to produce the same adaptive response that lower intake achieved in younger years. Harvard Health Publishing has synthesized the emerging consensus: protein needs for older adults likely exceed the current Recommended Dietary Allowance, which researchers established primarily from data on younger populations.
Sleep, seven to nine hours for most adults consistently, is not recovery from effort. It is the biological context in which muscle repair, metabolic regulation, cognitive consolidation, and hormonal cycling occur. Chronic sleep restriction systematically undermines every other healthspan investment simultaneously. Treating sleep as the substrate rather than a variable produces a different set of decisions than most midlife adults currently make.
Chronic stress carries measurable physiological consequences: elevated cortisol, accelerated cellular aging markers, and disrupted metabolic and immune function well-documented across multiple research frameworks. Stress elimination is not realistic in a demanding midlife life. Stress regulation through consistent physical activity, sleep, meaningful social connection, and deliberate recovery is a load-bearing component of any functional aging strategy.
What to Stop Doing Removal Practices Matter as Much as Additions
Sustained sedentary behavior carries independent metabolic consequences even among adults who exercise regularly. Chronic alcohol use disrupts sleep architecture, muscle protein synthesis, and liver metabolic function in ways that directly undermine the domains healthspan depends on. Habitual sleep restriction, even by amounts that feel manageable, produces cumulative cognitive and metabolic deficits compounding across months and years.
These are not costs that resistance training sessions fully compensate for. The removal side of the behavioral ledger receives almost no attention in mainstream healthspan content and may matter as much as the additions. What you stop doing accumulates in its own direction.
What Healthy Aging After 40 Is Not
The majority of commercially visible healthspan content exists primarily to sell products. Longevity supplements NMN, resveratrol, NAD+ precursors, senolytic compounds, and a rotating cast of others occupy enormous search space in this category with marketing language that substantially exceeds the human clinical evidence behind them.
Why the Most Marketed Longevity Practices Have the Weakest Human Evidence
Most longevity supplement research with compelling findings rests on animal models. Translation to human clinical outcomes requires randomized controlled trials with sufficient duration, sample size, and independent replication. For the majority of heavily marketed compounds, those trials either do not yet exist or have produced inconsistent results. Animal model findings are scientifically interesting and worth following as the research develops. They are not equivalent to human clinical validation, and the marketing does not reliably make that distinction.
Cochrane reviews and systematic analyses of specific compounds consistently note that evidence in healthy human adults remains preliminary at best. This matters for adults in midlife making real decisions about where to invest time, money, and behavioral energy.
What the Research Actually Supports and Why It Requires Less Than It Is Sold as Requiring
The evidence base for protecting healthy aging points, with remarkable consistency across multiple decades of research and multiple institutional sources, to a small number of behavioral practices requiring neither clinical infrastructure nor significant financial investment: consistent resistance training, sustained aerobic conditioning, adequate protein intake, prioritized sleep, and stress regulation embedded in daily life.
This is not a message that supports a supplement industry. It is, however, what the research supports. The distance between what the evidence recommends and what the industry implies you need is itself a finding worth sitting with.
Applying This in a Real Midlife Life
The 54-year-old who has been meaning to start for years and now encounters the first measurable evidence that waiting has carried a cost is not starting from zero. They are starting from wherever they are, with whatever constraints they genuinely have. That is the only available starting point, and it is sufficient.
The Minimum Effective Dose for Each Healthspan Domain
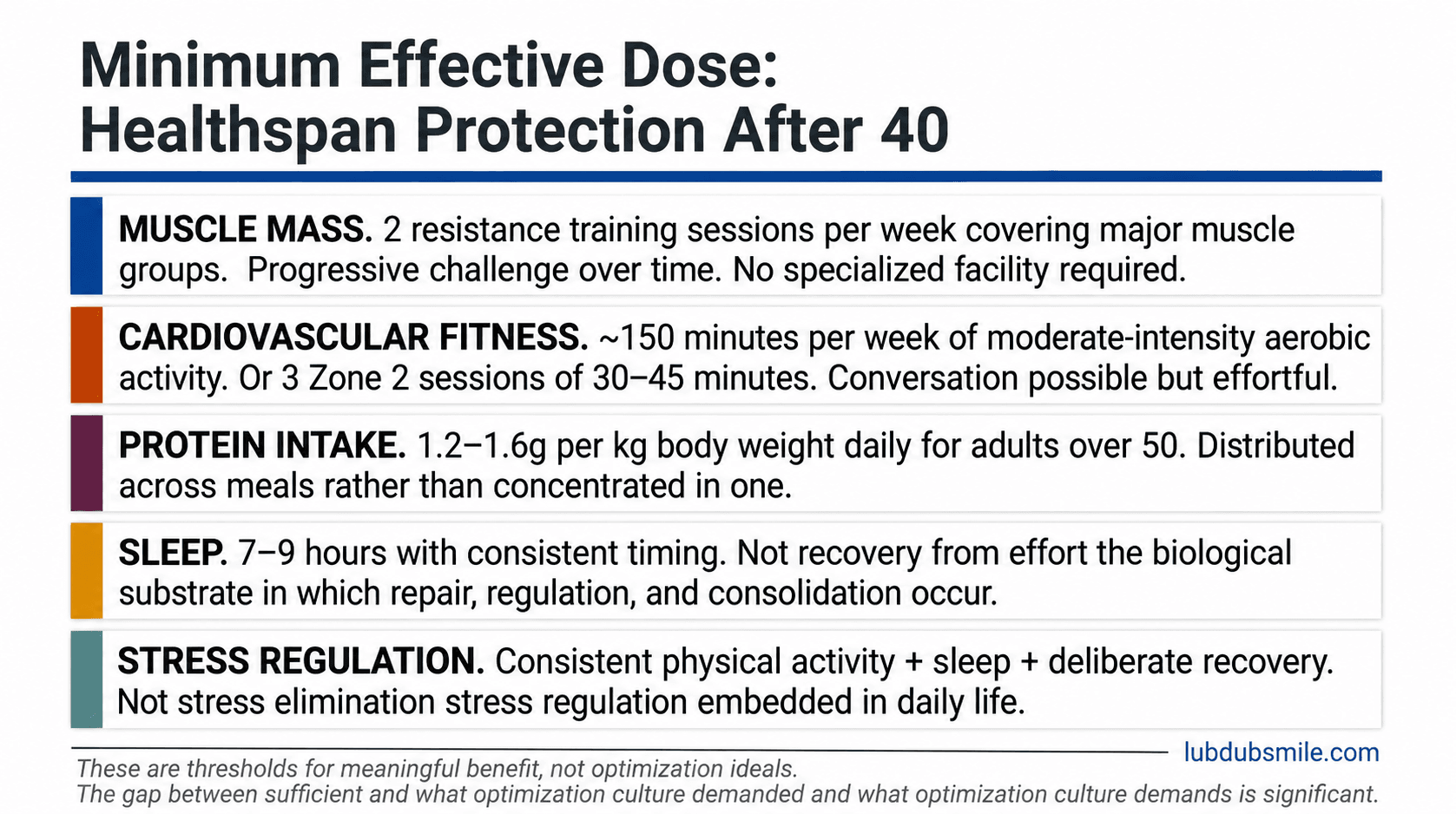
For generally healthy midlife adults, the evidence supports the following thresholds as sufficient to meaningfully protect key healthspan domains:
- Muscle mass: Two resistance training sessions per week covering major muscle groups with progressive challenge over time
- Cardiovascular fitness: Approximately 150 minutes per week of moderate-intensity aerobic activity, the Physical Activity Guidelines for Americans threshold, or three Zone 2 sessions of 30 to 45 minutes
- Protein intake: Approximately 1.2 to 1.6 grams per kilogram of body weight daily for adults over 50, distributed across meals
- Sleep: Seven to nine hours with consistent timing
- Stress regulation: The consistent presence of the practices above plus deliberate recovery time
Healthspan after 40 urgency is most felt watching a parent’s contracted capacity knowing the accumulation began long before it became visible.
These are thresholds for meaningful benefit, not competitive standards or optimization ideals. The gap between what is sufficient and what optimization culture demands is significant. Conflating the two is a primary driver of the overwhelm that keeps midlife adults in intention without action. For many adults navigating demanding careers, active parenting, and the competing claims of midlife, the minimum effective dose is the honest and appropriate target.
Where to Start When You Have Been Meaning to Start for Years
Start with the domain where the minimum effective dose feels most achievable and the functional return is most immediately relevant. For most sedentary midlife adults, resistance training provides the highest-leverage entry point because muscle mass protection compounds most significantly over the years ahead and because entry-level resistance training requires no specialized facility and minimal time.

The concern that it is too late is understandable and almost universally overstated. Research on adults initiating resistance training in their 50s and 60s demonstrates meaningful muscle adaptation, not identical to what was possible at 35, but significant relative to declining trajectories. The accurate framing is not that it is too late. It is that the return on starting now is lower than it would have been at 40 and higher than it will be at 65. For most people reading this, that window remains genuinely open.
Pairing that entry point with sleep protection and consistent protein intake creates a behavioral foundation that addresses multiple healthspan domains simultaneously without requiring a restructured life. Understanding how relationships strengthen health adds a further dimension that the exercise literature alone tends to underplay. Social engagement and emotional connection carry independent functional aging benefits that belong in the same conversation.
The Midlife Window Why Functional Aging Investment Has More Return Now Than It Will at 65
This is the biological argument that most healthspan content does not make with sufficient specificity. It is the one that most changes how the behavioral recommendations above feel, from general good advice to personally urgent decisions.
What the Research Shows About When Behavioral Change Has the Most Biological Return
Longitudinal intervention research consistently shows that muscle mass responds to training across a wide age range, but that the rate of adaptation and the starting reserve both decline with age. A midlife adult beginning resistance training at 48 starts from a higher muscle mass baseline, adapts more rapidly, and has a longer timeline over which the protective effect compounds than the same adult beginning at 65.
VO2 max shows similar patterns. The Annals of Internal Medicine has examined midlife behavioral change and its association with later-decade functional outcomes, finding that the magnitude of long-term benefit closely relates to when the behavioral pattern shift occurred. Earlier investment produces compounding return. Later investment produces meaningful benefit but from a lower starting position and across a shorter horizon.
How Compounding Return Works and Why the Timing of Investment Matters More Than Its Intensity
The compounding principle operates in both directions. The physiological mechanisms that produce accelerating decline when behavioral patterns stay sedentary also produce accelerating benefit when behavioral patterns shift. An adult who begins resistance training at 48 does not simply add two decades of training before reaching 68. They arrive at 68 with a meaningfully higher muscle mass baseline, better metabolic flexibility, and a cardiovascular fitness reserve that makes subsequent aging less steep.
The same hour of effort, applied twenty years earlier, does not produce the same linear output. It produces compounding return that restructures the trajectory the later decades operate on. This is the argument most longevity content obscures with supplement marketing and optimization culture. The behavioral investments with the highest return are the ones made now, with the tools already available, within the life already being lived.
Adults beginning this process often find that the emotional and identity dimensions of midlife health work are as significant as the physical ones. The work of redefining strength after 40 and understanding emotional regulation as a daily skill both belong in the same framework as resistance training and protein intake. Functional aging is not only a physical project.
Healthspan After 40 Is Not a Future Project
The practices that protect functional quality of life in later decades are not aspirational. They are available, they do not require clinical tracking systems, supplement protocols, or elite intervention infrastructure but they require resistance training twice a week, enough sustained cardiovascular effort to maintain aerobic base, protein distributed across meals, and sleep treated as the non-negotiable substrate it is.
What most longevity content will not state plainly is that the distance between where most midlife adults currently stand and where the minimum effective dose would place them is not as large as the industry implies. The practices are not complicated. The window for compounding return on healthspan after 40 is not closed. Every decade of consistent behavioral investment in muscle, cardiovascular fitness, and recovery accumulates in the direction of function rather than away from it.
The recognition that living longer was never the whole goal is the beginning of the question. The behavioral framework for protecting what fills those years is available right now, without waiting for a better moment, a better protocol, or a better version of your schedule.
Understanding what the preventive health landscape recommends at each decade, how metabolic health and healthy aging interact over time, and why emotional hygiene belongs in the same behavioral framework as exercise and nutrition rounds out the picture that the functional aging literature increasingly supports. These are not separate projects. They are facets of the same sustained investment.
This content is for educational and informational purposes only and does not substitute for advice from a qualified medical, psychological, therapeutic, or legal professional.